


Universities UK is not the first sector body to analyse the sector impact of the NHS Workforce plan.
It’s long been clear that the doubling of places for student doctors (with 500 new places by 2025) and nurses – albeit with steady growth rather than a single allocation, and some tinkering around the edges on other modes of delivery – will have a huge impact on the universities that deliver them.
From plan to reality
Equally clear has been the need for this expansion to be thoughtful and strategic, and to come with a parallel increase in the number of available NHS placements. Delivery of such expansion might mean new partnerships, and new approaches to teaching – these need to be carefully considered and scaled given the numbers and costs involved.
And simply pumping students and newly qualified professionals into a system that may not be set up to manage this would cause problems – the longer term increase in NHS salary costs, for instance, needs to be considered. The Institute for Fiscal Studies put the cost of salaries at around £50bn in today’s terms by 2026-27, on top of the £2.4bn already factored in for training new staff.
However, the public is in favour of expansion. Recent Public First polling found that 30 per cent of UK adults saw the expansion of spending on courses like medicine as a key priority for any future allocation to higher education – rising to 41 per cent of the over 65s, and 37 per cent of Conservative voters. There’s clearly a political consensus in favour of expansion too.
For providers themselves, the complexity of regulatory regimes around healthcare provision are nearly as daunting as the capital costs of building capacity, and the recurrent costs of staffing to run it. The whole thing is a huge ask of the sector – but there is one issue that needs urgently addressing first.
Who wants to work in healthcare?
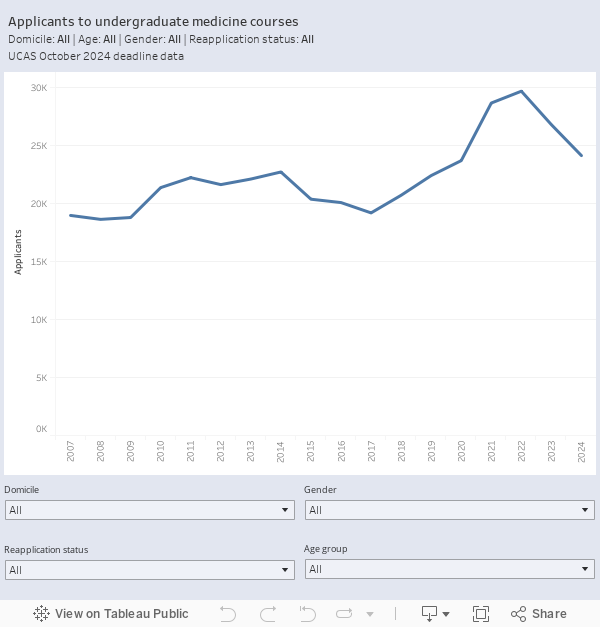
The inconvenient truth is that applications (not even student numbers – applications) for medicine and nursing are falling. Data from the October 2024 UCAS deadline shows applications to medical schools falling for the third year in a row.
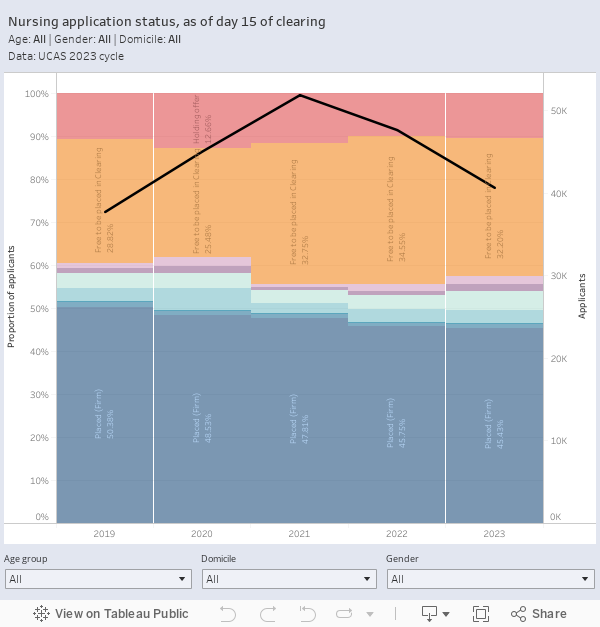
And similarly, in nursing, clearing day 15 data shows a two year decline has returned applicant numbers to a pre-pandemic level. Incredibly, the proportion of applicants placed at their firm choice provider has fallen for five straight years (though there has been a corresponding small growth in clearing).
We also need to think about the student experience and student attrition. A recent report (Clinician of the Future 2023: Education Edition, based on a survey of 2212 medical and nursing students globally) from Elsevier found that 21 per cent of UK medical students are considering quitting their course – with 76 per cent worried about the costs of their studies. Both these are substantially above the global average.
But the perception of a career riven with staff shortages and unrelenting workload is strong – 75 per cent of medical students are worried about clinician shortage, and 65 per cent of nursing students are worried about burnout. The consensus seems to be that the prospect of a future involving low pay and poor working conditions is starting to cut through among potential applicants and current students.
Unfortunately, not all of these students will make it through the course. Research from the Nuffield Trust suggests that one in eight nursing students did not complete their intended degree between 2014 and 2020, and one in nine midwifery students do not join the profession on graduation. Data is harder to come by on the totality of the medical training pipeline, but it seems that for every one fully-qualified general practitioner we need to offer two training posts.
The plan put forward by Nuffield focuses on student loan forgiveness in return for years of NHS service, covering nurses, midwives, and allied health professionals. This may increase application numbers, student retention, and graduate progression to the NHS – but it is another expensive ask on top of what has already been promised and requested (though there are suggestions that the cost and savings would cancel out).
State of the nation
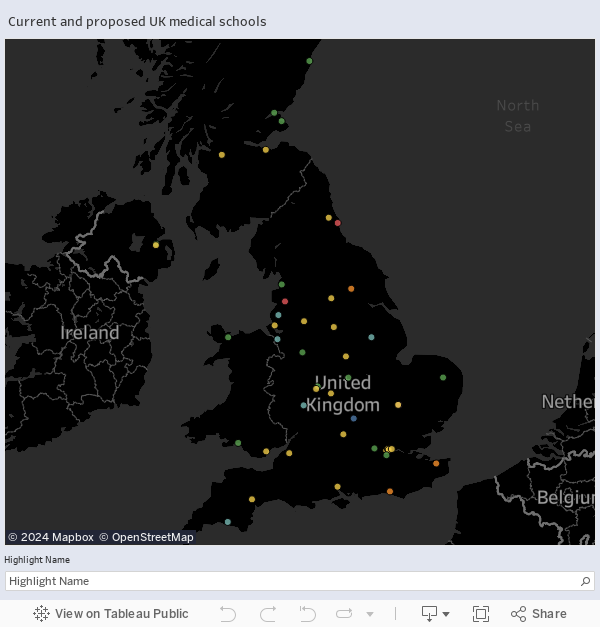
There have been many recent expansions in the availability of funded places, and indeed in the number of UK medical schools. Here’s how things look currently.
In terms of the numbers of medical and related students in each provider, the available HESA data is not quite the last word (the vagaries of subject coding apply even at the fairly detailed CAH level three). But this is the state of play in a sample of likely looking codes.

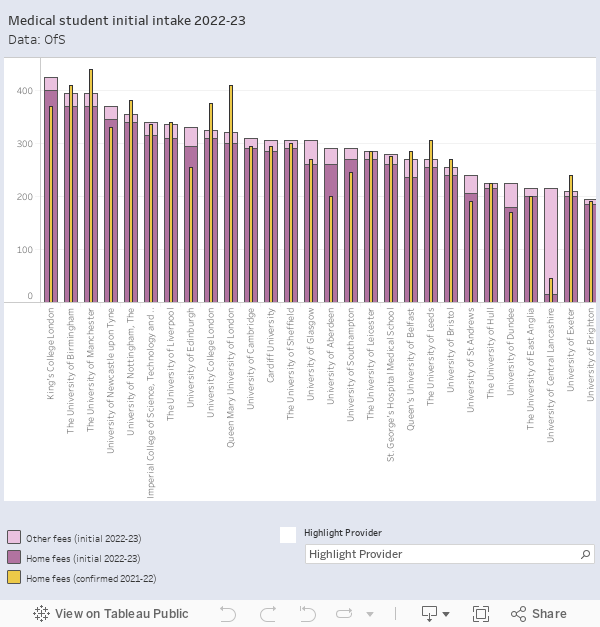
The Office for Students publishes data for medical recruitment across the UK. This chart shows the number of home fee paying and non-home fee paying (usually overseas) medical students initially accepted at each provider in 2022-23 – the thinner yellow lines show confirmed home intakes (minus those who leave the course) in 2021-22. If you’ve spotted that the institution names don’t quite match the map at the top, be aware that three of the four joint medical schools (Brighton/Sussex, Hull/York, Kent/Canterbury) submit joint returns, whereas the University of Nottingham returns numbers for it’s own medical school separate from the joint Nottingham/Lincoln operation.
Asks in context
The UUK request for a government-funded campaign to promote the variety of careers (and new and existing routes into these careers) feels like a bare minimum given what appears to be happening to applications. It does feel like we are looking at a demand-side problem. There’s little indication that the current dash for short, modular, courses would achieve much in healthcare given the need to address (rightly) rigorous professional standards. And although an apprenticeship route is welcome, the amount of apprenticeship attrition and the likely low numbers involved don’t look likely to move the dial.
We will clearly need more educators within universities, but this in itself would pull experienced staff away from the front line and thus from placement provision. On the latter there are clearly huge capacity issues that also have an impact on patient care. Likewise, there is potential in using new technologies to support training capacity – but there will always be a need to get patients and students interacting, and for this to be properly supervised and supported.
Fundamentally, healthcare education is a balancing act between a number of different pressures. We’re dealing with the impact of more than a decade of underinvestment, and there are no easy or quick fixes. Universities are standing up to provide the training and support the healthcare sector needs, but in return need to be properly supported themselves – with long term, consensus-driven, plans and steady, dependable, resource increases.











For nursing, and of course many other roles in the NHS, FE colleges could do so much more with the right support and investment. It has taken several years for one college to gain permission to deliver nursing degrees, in a (very) cold sport area, in partnership with a university. We need more colleges to be able to do that. Plus we need a proper partnership between colleges and universities in every place with their NHS trusts – enabling the employers to have a one-stop offer across all of their workforce. Sadly, the narrow focus on doctors and nurses, important though it is, will result in the NHS not having all of the other staff it needs.
The suggestion:
“The plan put forward by Nuffield focuses on student loan forgiveness in return for years of NHS service, covering nurses, midwives, and allied health professionals. This may increase application numbers, student retention, and graduate progression to the NHS”
isn’t borne out in Scotland, where there is a £10,000 annual bursary on top of free education. We have no better stats than England (probably worse). My university has targets from the Scottish Government, and in 2022 we were 11% under, and in 2023 around 20% under. Despite every effort. There are not the people who want to be nurses, even if they are paid £10k to do it. Our retention isn’t any better either.
The number of University medical student places in Scotland seems to be higher than in England as a percentage of the 2 populations. If there are vacancies for training in Scotland, it seems a waste, given that over 50% of applications for Medicine to English Universities are unsuccessful, even though many have the necessary UCAS points for entry.
Perhaps there should be a special clearing platform between the 2 countries to maximise the places on offer?
Medical graduates are some of the highest paid graduates in the UK and can earn even more if the go and work abroad in USA or Australia.
I think it is very dangerous to offer bonus payments upfront to those being trained for jobs in the medicine and related sectors in England. The costs to Universities (and the taxpayer) are much higher than the £9,250 a year loan the student has to carry forward. They already have a very good deal.
Perhaps the children who’ve gone on to become students on nursing courses have been telling their younger siblings and friends just what a s-show it and working for the NHS is? The recent TicTok flurry of video’s of young individuals bemoaning starting work working for a living 9-5 is a perfect example of the uphill struggle in many sectors to retain young staff, and the stress of NHS ‘graduate’ nursing training coupled with shift working, and not spending several years arse wiping and learning interpersonal skills as nurses did in the past, make the ‘adulting’ aspect even harder.
Then there’s the EDI issues, especially for MALE student nurses, for whom it’s a near constant battle to prove themselves worthy to female nursing lecturers who still see it as a purely female career…
We need to be working in partnership with the (relatively newly created) Integrated Care Boards if we are to come any where near to realizing the ambition of the workforce plan. This join up is currently a missing part of the jigsaw.
There are of course ‘asks’ of the current education providers – the HE institutions themselves. However, my recent close up experience of one large provider is that there is poor management of the academic teaching delivery with far too little face to face engagement of student nurses. So when people who do care for others and consider themselves ‘people focused’ start to study on a Nursing course it is no wonder they drop out if they have little face to face time to become part of a team and properly engage. HEIs can significantly help this situation in the short term.
Expanding health education provision is no longer a choice but a mandate. Aligning with recent sentiments, I wholeheartedly endorse the call for new partnerships and innovative teaching approaches. The transformation of medical education is a vital convergence of opportunity and necessity.
If we are to enable scaling health education while elevating its quality and efficiency we must address the critical barriers to increasing the student numbers on programmes. For example:
1) Improve the teaching and training experience for clinicians and health educators.
2) Increase and augment placement opportunities on offer to accommodate the extra number of students.
3) Provide programme flexibility e.g. adaptive, competence based and recognise prior learning thus attracting a more diverse cohort of students, including existing healthcare professionals.
Innovative technologies have driven huge productivity improvements in healthcare and other sectors, while it has remained broadly flat in medical education.
Adopting proven technologies can help address the above barriers; scale training in clinical practice and offering flexible and adaptive programs. Such innovations can improve the teaching experience and improve access. Modernizing health education extends beyond technology. It’s vital to envision a long-term, flexible approach to lifelong learning and workforce development.